Heart Attack Risk Factors: What You Need to Know
28 February 2020

All too often we hear of someone we know- dying suddenly, without warning, which prompts self evaluation and temporary efforts to address our diet and lifestyle in the hope of preventing a similar affliction to ourselves. It is not uncommon to start ‘feeling’ symptoms of chest pain and breathlessness resulting in visits to the doctor to get reassurance that you are free of heart disease.
In the course of this article I hope to help you understand what it is that gives rise to these nightmare scenarios and how to avoid them – with a sensible and sensible approach.
Major Heart Attack Risk Factors
Most people with sudden cardiac death or heart attack have A REASON for it i.e. underlying risk factors that were either unrecognized or inadequately managed.
The key underlying major risk factors are:
- family history of premature coronary disease
- diabetes
- hypertension
- smoking
- hyperlipidemia (high cholesterol)
Low HDL cholesterol <1 mmol/l or 40 mg/dL (low ‘good’ cholesterol), sedentary lifestyle, obesity and stress are amongst the less important risk factors.
There has been extensive scientific evidence that by identifying these entities early and treating them aggressively, heart attack and stroke can be significantly reduced. The duration, severity and coexistence of these risk factors contribute cumulative risk.
In my opinion, family history is the most important risk factor. If you have a father with proven coronary disease before the age of 55 or mother before 65, you are at increased risk even if you have no other risk factors.
Take Action Now by Getting Screened.
A full blood profile including fasting blood sugar and lipids (cholesterol profile) should be done before the age of 30 to ensure that the coronary risk environment is optimal.
Individuals frequently become alarmed when they go to chemistry labs to check their own bloods and find their levels are outside the printed recommended safe levels. It is important that these results are interpreted by a clinician who can put those results into perspective. With regards to lipid (cholesterol) levels there are prescribed targets that are recommended depend on the rest of the prevailing risk factor burden. e.g. If you have had coronary disease, a previous leg artery blockage, diabetes or stroke, the target LDL level should be <2.6 and if you have two or more of the above major risk factor listed above then the target should be below 3.4 (130 mg /dL). The total cholesterol which is what most people appear concerned about is less useful to decide on risk.
Diabetes is a very serious metabolic condition that has wide-ranging harmful effects. Unfortunately, damage to heart, brain and other medium sized vessels occurs early in the metabolic process before the blood sugar reaches levels that are called diabetes (fasting sugar>7 mmol/L). High blood sugar over time eventually leads to small vessel damage and usually manifests with kidney failure, nerve and retinal eye damage which can lead to blindness. Hence the recommendation for regular blood sugar measurements especially where there is a family history of diabetes.
Due to the associated adverse vascular damage in these individuals, stringent BP targets of 130/80 and LDL cholesterol targets of 2.6mmol/L or <100 mg /dL are recommended.
Hypertension is common and is prevalent in as much as 1/3 of the adult population and represents a major cardiac risk factor. The target blood pressure for everyone regardless of age is <140/90 except for diabetics or those with kidney disease where the target is 130/80.
Adopt a healthy diet and lifestyle
If you do have any of these risk factors it is very important that you adopt a healthy diet and lifestyle. If the target prescribed safety levels are not attained after a reasonable attempt has been made, commencement on medications is required. It is extremely unlikely that drug treatment can be stopped as their effect is purely suppressive of the underlying basic abnormality. One should be aware that long term drug treatment in these conditions is not only safe but has been clearly shown to reduce risk and prolong life. One of the most common mistakes we see is patients stopping medication when the cholesterol level has dropped to a satisfactory level in the hope that it has been cured. This is completely wrong.
The incidence of a heart attack is increased about sixfold in women and threefold in men who smoke compared to subjects who have never smoked. The reduction in cardiac risk associated with smoking cessation is rapid and nearly approximates the risk of non smokers after 5 years.
How Do I Check My Heart Condition?
If you don’t have any of the above risk factors and you have no symptoms then there is little reason to go further to specifically test your heart. However, if you fulfill one or more of those criteria, you would be advised to seek medical attention especially if you start experiencing symptoms such as exertional chest pain or breathlessness.
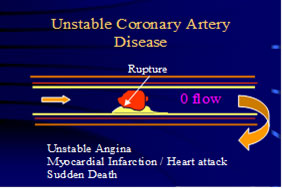
Risk factors translate into heart risk via the formation of coronary plaques.
Now, techniques exist for the quantification of plaque and hence estimations of risk. Plaques that gradually accumulate at a particular location may, if severe, produce narrowing of the vessel, and thus symptoms such as chest pain and breathlessness with exertion. It is called stable angina. On the other hand these plaques even when mild, if soft and are cholesterol rich develop inflammation may rupture and give rise to a local blood clot which could lead to heart attack (a situation akin to a burst pimple on the inside of the blood vessel).
Exercise stress testing in people has little value when performed in low risk individuals with no symptoms. Exercise testing will only detect the presence of a severe narrowing in a coronary artery ~70% of the time and these severe stable narrowings rarely cause heart attack. Paradoxically, most heart attacks and sudden death are caused by mild narrowings <50% which are not detectable by exercise testing. Thus it is not rare to find examples of heart attacks occurring in people who have had normal stress tests.
On the other hand, 30-40% of individuals (especially females) who have perfectly normal heart arteries may have abnormal or positive stress tests.
Calcium score assessment using multislice /EB CT technology provides additional information in assessing individuals who are at intermediate risk of heart disease. Calcium deposition occurs where plaque develops in the heart arteries and is proportional to the amount of disease.
Computerized tomographic (CT) coronary angiography (non-invasive angiography) using multislice scanners are currently available in Malaysia and allows visualization of the coronaries including calcified and non calcified (soft) plaques. This technology provides good visualization of mild and severe plaques and helps the physician to make sound management decisions.
High-risk individuals with clearly abnormal (positive) exercise tests, proven heart events with classical symptoms should not be doing these scans and instead should undergo conventional invasive angiography with a view to treating the problem at the time.
My personal view is that individuals who have low risk of heart disease (few or no risk factors) who have an abnormal stress test or individuals with risk factors who complain of symptoms that are not typical of heart, are appropriate candidates for non-invasive angiograms thus avoiding unnecessary invasive procedures. The role of screening asymptomatic high risk individuals with non-invasive angiography is still a subject of controversy.
Individuals with heavy calcium deposits in their arteries (which increases especially with age), fast or irregular heart beats do not make good candidates for scanning due to artifacts that mar the accurate interpretation of results. In my opinion concerns about radiation exposure are overstressed because these are one-off procedures which yield useful information with an estimated additional lifetime hazard of cancer of about 0.07%. At the same time routine CT angiogram screening / surveillance especially in low risk individuals is definitely discouraged.
Thus for a road map to good cardiovascular health in to old age, identify your personal risk status early, be compliant with prescribed medications if deemed necessary and seek medical advice early to get the appropriate tests performed to prevent complications.
Tags: heart
Back
